Neuroscience, Personalized Medicine
What is dopamine?
Dopamine is a neurotransmitter, a chemical that shapes how the brain processes information. It does this by binding to different categories of dopamine receptors which then leads to changes in the intracellular processes of neurons, the cells responsible for transmitting information in and outside the brain. The D1 family of dopamine receptors (D1 & D5) increase intracellular levels of a chemical second messenger, cyclic AMP, which can then affect how a neuron processes other signals it receives. The D2 family of dopamine receptors (D2, D3, & D4) decrease cyclic AMP, which can also shape neural responses. How the dopamine signals interact with other signals in the brain can be quite complex and is beyond the scope of this piece. For more see this review article.
Dopamine signaling plays a role in a variety of critical cognitive processes including motor control, learning, and decision making. It has also been implicated in the addictive nature of drugs of abuse, which I studied in some detail during my Ph.D. and postdoctoral research.
Dopamine signaling plays a role in a variety of critical cognitive processes including motor control, learning, and decision making. It has also been implicated in the addictive nature of drugs of abuse, which I studied in some detail during my Ph.D. and postdoctoral research.
Positron Emission Tomography and measuring dopamine signaling in the human brain
Positron Emission Tomography (PET) allows scientists to measure dopamine signaling in the living brain. PET has been around since the 1960s and involves imaging the location and amount of a radiotracer (radioactively-tagged compound) in the body. Most PET radiotracers contain C-11, F-18, or O-15 radioactive isotopes. These isotopes release positrons (which are the antiparticle of the electron) which, when they interact with nearby electrons in the body produce an annihilation event leading to 2 gamma ray photons being emitted at 180 degrees. The PET scanner "counts" these gamma ray events and ultimately reconstructs the image that produced the events by projecting the gamma ray counts back into the body part being imaged. These PET images give quantifiable data regarding the amount of tracer that accumulates in a particular area over time.
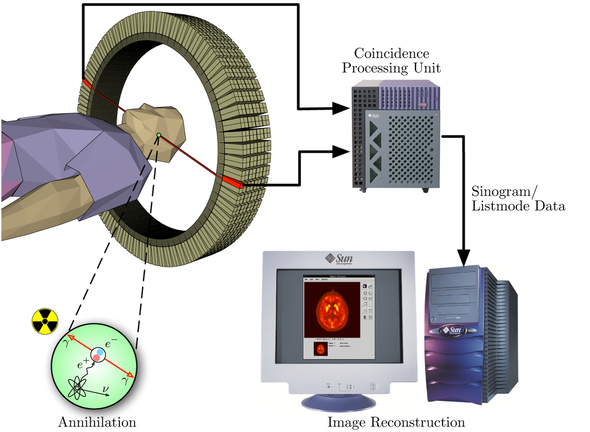
Schematic of how a PET scanner measures gamma rays to quantify the level of a radiotracer in particular anatomical areas of the brain. Image by Jens Maus (http://jens-maus.de/); Public Domain, https://commons.wikimedia.org/w/index.php?curid=401252
Brain PET is a particularly powerful technique in that we can use radiotracers that allow us to investigate brain metabolism, neurotransmitter receptors (dopamine or opioid, among others), neurotransmitter synthesis, and the presence of beta-amyloid plaques (often present in Alzheimer's disease). With these compounds we gain a better understanding of individual differences that may be useful as markers of disease state or risk for developing a particular disease. Common radiotracers for imaging the dopamine system include FDOPA, C-11-Raclopride, F-18-Fallypride, FMT, and others. Several groups have used some of these compounds to better understand the dopamine system's role in drug abuse.
Do dopamine signaling differences reflect risk for drug addiction?
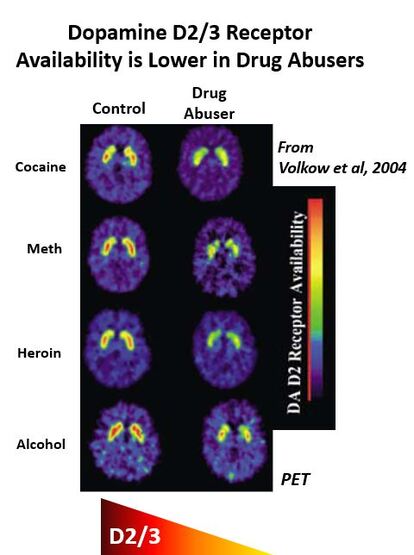
All drugs of abuse release dopamine in the brain. Dopamine, among other things, links pleasure/wanting with the stimuli its release is paired with. Thus, differences in dopamine signaling in response to drugs of abuse may relate to a greater propensity to re-use drugs found to be rewarding and potentially lead to increased risk for drug addiction.
PET imaging has shown that lower dopamine D2/3 receptors are present in a variety of drug-addicted individuals (alcohol, cocaine, methamphetamine, heroin) when compared to healthy controls. Whether low D2 receptors are a cause or consequence of problematic drug use has been difficult to determine in human studies, however.
PET imaging has shown that lower dopamine D2/3 receptors are present in a variety of drug-addicted individuals (alcohol, cocaine, methamphetamine, heroin) when compared to healthy controls. Whether low D2 receptors are a cause or consequence of problematic drug use has been difficult to determine in human studies, however.
Animal work has suggested that behavioral impulsivity is associated with lower D2 receptor levels in rodents. These researchers also found that high impulsive rats would later go on to self-administer more cocaine than low impulsive rats (Dalley et al., 2007). Thus, D2 receptors may confer a greater propensity to engage in behaviors that are associated with drug addiction risk in humans (impulsivity, novelty seeking). Furthermore, work in non-human primates has shown that low D2 receptor levels predict escalation in cocaine self-administration, which leads to lower D2 receptor levels (Nader et al., 2006). This work suggests that low D2 receptor levels may predispose individuals to escalate drug use and that chronic drug use further changes these receptor levels.
Human PET studies have focused on individuals with a family history of addiction to try to corroborate the animal work linking dopamine D2 receptors with addiction risk. Volkow et al. 2006 have shown that individuals with a family history (FH) of alcoholism show heightened striatal (a region deep in the brain responsible for reward processing, learning, and action initiation) D2 receptor levels compared to subjects without a family history. They argue these high D2 levels may serve as a protective factor that prevented these individuals from becoming alcohol abusers themselves. This finding highlights the complexity of working with human subjects as the animal literature might have suggested the opposite finding (lower D2 in FH individuals). Human motives to use drugs are many and often the environment greatly shapes behavior. It could be argued that FH positive individuals with lower D2 (not observed in Volkow et al) had behavioral profiles (see Dalley et al., 2007; above) that resulted in them already transitioning to alcohol/drug abuse and thus being excluded from the Volkow study. Undoubtedly, there are more variables associated with risk for drug use than low D2 levels and future work may be able to identify what other factors (genetic, environmental, social) interact with D2 levels to predict drug abuse risk.
Genetic factors affecting dopamine signaling
There has also been interest in understanding whether genetic differences may lead to different levels of D2 receptor availability, potentially placing some individuals at greater risk for addictive disorders. I investigated the effect of some common D2 receptor single nucleotide polymorphisms (SNPs) on D2 receptor availability using F-18-Fallypride as part of my postdoctoral research. Many of these SNPs had been previously associated with dopamine receptor differences in relatively small PET studies or been associated with potential increased risk for drug addiction.
- Taq1A - A1 allele associated with lower striatal D2 receptor availability (replicated in separate study but not in a third)
- C957T - C allele associated with lower striatal D2 receptor availability in study of 45 individuals
- -141C Ins/Del - inconsistent findings on whether it affects D2 receptor availability
Since the Taq1A SNP was discovered to associate with differences in dopamine signaling first, researchers have used it as a proxy for D2 receptor status (or more loosely as an index of general dopamine functioning). However, given that the Taq1A polymorphism does not occur within the DRD2 gene itself, researchers have speculated that polymorphisms in Taq1A may associate with other SNPs in the DRD2 gene that are the real drivers of expression of the receptor in vivo.
The C957T and -141C Ins/Del polymorphisms are in strong linkage disequilibrium with Taq1A and have themselves been associated with striatal D2/3 receptor availability. Despite the data suggesting that these SNPs are strongly linked, few studies have systematically investigated the effect of C957T, -141C Ins/Del, and Taq1A in isolation and combination on D2/3 receptor availability. Beyond the potential link to drug addiction risk, characterizing the functional effect of these SNPs on D2/3 receptor availability has implications for better understanding the mechanisms through which they exert their demonstrated influence on motivated behaviors including learning and decision making, impulsivity, and reward responsivity.
In our work, we used F-18-Fallypride, which is a D2/3 receptor tracer with favorable affinity to measure both striatal and extrastriatal dopamine receptors, and assessed the impact of C957T, Taq1A and -141C Ins/Del SNPs on D2/3 receptor availability in a sample of 84 healthy subjects.
The C957T and -141C Ins/Del polymorphisms are in strong linkage disequilibrium with Taq1A and have themselves been associated with striatal D2/3 receptor availability. Despite the data suggesting that these SNPs are strongly linked, few studies have systematically investigated the effect of C957T, -141C Ins/Del, and Taq1A in isolation and combination on D2/3 receptor availability. Beyond the potential link to drug addiction risk, characterizing the functional effect of these SNPs on D2/3 receptor availability has implications for better understanding the mechanisms through which they exert their demonstrated influence on motivated behaviors including learning and decision making, impulsivity, and reward responsivity.
In our work, we used F-18-Fallypride, which is a D2/3 receptor tracer with favorable affinity to measure both striatal and extrastriatal dopamine receptors, and assessed the impact of C957T, Taq1A and -141C Ins/Del SNPs on D2/3 receptor availability in a sample of 84 healthy subjects.
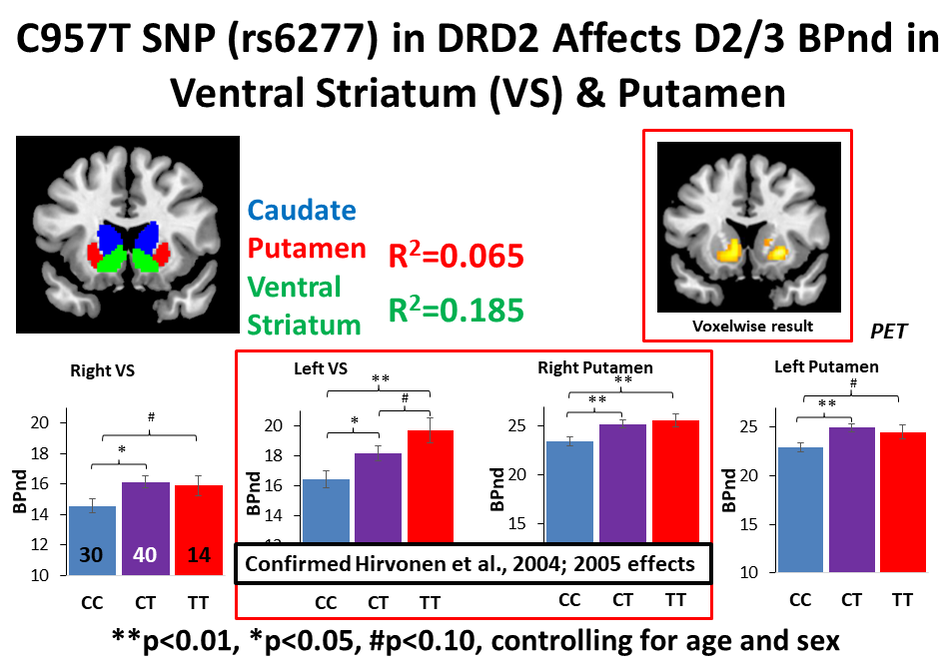
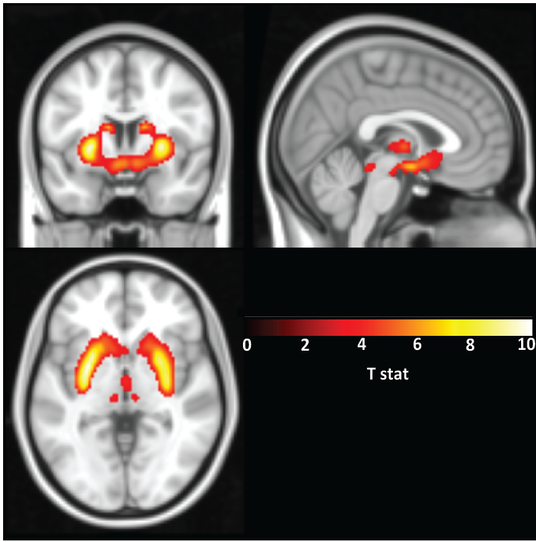
The C allele of the C957T SNP was associated with lower D2/3 receptor availability in the ventral striatum and putamen. No other SNP investigated demonstrated an effect on D2/3 receptor availability. BPnd=binding potential, a measure of D2/3 receptor availability; VS=ventral striatum
We found that the C957T SNP was associated with variation in dopamine D2/3 receptor availability in areas of the striatum often implicated in reward processing. The fact that the C allele was associated with lower dopamine receptor availability suggests it could be a useful genetic measure for at least one biological factor (lower D2 receptor availability) linked with drug addiction. While more work needs to be done to confirm these results, certainly further study of the C957T SNP in the DRD2 gene is warranted.
Individual differences in dopamine release
Another area of focus regarding dopamine’s role in addiction is understanding differences in dopamine release to potential drugs of abuse. This measure is more closely associated with the biological processes associated with actual drug use, but is collected in a more controlled, laboratory setting. PET psychostimulant challenge studies allow researchers to examine dopamine release in the brains of human subjects. Methylphenidate and d-amphetamine (dAMPH) are often used in these PET studies as both release dopamine in the brain by blocking and/or reversing the dopamine transporter. If PET radiotracers that are displaceable by endogenous dopamine are used, researchers can perform a PET scan after placebo or psychostimulant administration and measure the change in radiotracer signal. The PET signal will go down after a psychostimulant for a tracer that is displaceable as the increased endogenous dopamine released by the drug lowers the binding sites for the tracer in the brain. This change in binding potential of the radiotracer can be used as a measure of dopamine release and has become a useful tool in research into addiction related processes.
Areas of significant change in D2/3 receptor availability as measured by F-18-Fallypride PET after dAMPH administration when compared to PET data collected on placebo. This change in receptor availability on dAMPH is interpreted as a measure of the level of dopamine release to the dAMPH. Data from 34 healthy young adults. dAMPH=d-amphetamine
Using this PET technique, Casey et al 2014 found that young adults with a multigenerational FH of substance use disorders showed reduced dAMPH-induced dopamine than either healthy controls or subjects that personally used drugs at similar levels to the FH group but without a FH of substance use disorders. This study was particularly informative as the effects of current drug use were also investigated and measured separately from family history. Furthermore, our group and others have demonstrated that dAMPH-induced dopamine release correlates with subjective ratings of the drug, particularly wanting more, in drug naïve individuals. These data confirm animal work linking changes in dopamine signaling after drug use to wanting processes (which has been labeled incentive salience).
Read more about wanting, liking, and drug abuse in a previous blog post.
The concept of blunted dopamine signaling (lower D2 receptor levels and less dopamine release) as biomarkers of addiction has also been recently reviewed (Trifilieff et al 2017; Leyton, 2017). While more work needs to be done, understanding factors that influence these PET-based biomarkers of dopamine signaling in human subjects has the potential to identify at risk individuals. This risk identification may allow intervention to be attempted earlier in the addiction process or perhaps prevent addiction before it even occurs.
Read more about wanting, liking, and drug abuse in a previous blog post.
The concept of blunted dopamine signaling (lower D2 receptor levels and less dopamine release) as biomarkers of addiction has also been recently reviewed (Trifilieff et al 2017; Leyton, 2017). While more work needs to be done, understanding factors that influence these PET-based biomarkers of dopamine signaling in human subjects has the potential to identify at risk individuals. This risk identification may allow intervention to be attempted earlier in the addiction process or perhaps prevent addiction before it even occurs.
Individual differences in dopamine signaling and the future of personalized medicine
The term “personalized medicine” has gained popularity in recent years. While it may seem like a buzzy term, its potential for improving treatment of a variety of medical conditions is vast. Personalized medicine involves tailoring treatments to individuals based on some aspect of their biology that might affect how they respond to a treatment. For example, you might give one patient with a particular genetic variant a different pharmacological treatment than another if that variant affects how they process (metabolize) or respond to that particular drug. This particular approach of using genetic information to understand response to pharmaceuticals is termed pharmacogenomics (see also).

The rapid reduction in the cost to sequence the human genome (complete set of an individual’s DNA) as well as proliferation of genotyping services such as 23andMe (which genotype common genetic polymorphisms, or areas in human DNA most likely to vary across individuals) means that genetic data can be readily obtained by anyone who wants it. This technological advance will allow physicians greater information of a patient’s underlying biology and eventually will be merged with growing insights into the effects of genetic variation on drug metabolism, brain signaling, and behavior to make personalized medicine commonplace. In fact, pharmacogenomic data has been added to several drugs by the FDA.
My own work, referenced above, suggests that genetic variation in a gene encoding the dopamine D2 receptor (DRD2) can affect the relative availability of this receptor in the brain as measured with PET (Smith et al., 2017 Translational Psychiatry). Individuals with a particular genetic variant in DRD2 that is associated with less availability of the receptor (C957T CC individuals) may need either a higher dose of a D2 drug or a higher affinity D2 drug to receive a therapeutic benefit.
The implications for this finding go beyond potential treatments or interventions for drug addiction. D2 agonists are commonly used in Parkinson’s Disease patients to preserve motor function and D2 antagonist-like drugs are used in the treatment of Schizophrenia. Understanding the genotype of individuals affected with these conditions, then, could enhance the effectiveness of their D2 drug treatments (by suggesting a physician might want to start with a higher or lower dose of the drug). While studies such as ours linking genetic variation with differences in biology are encouraging, DNA can also be modified by the environment. Researchers have begun studying these epigenetic effects on behavior, with most work occurring in rodents. As we integrate this knowledge, we will begin to better understand the impact gene by environment interactions have on biology and behavior.
My own work, referenced above, suggests that genetic variation in a gene encoding the dopamine D2 receptor (DRD2) can affect the relative availability of this receptor in the brain as measured with PET (Smith et al., 2017 Translational Psychiatry). Individuals with a particular genetic variant in DRD2 that is associated with less availability of the receptor (C957T CC individuals) may need either a higher dose of a D2 drug or a higher affinity D2 drug to receive a therapeutic benefit.
The implications for this finding go beyond potential treatments or interventions for drug addiction. D2 agonists are commonly used in Parkinson’s Disease patients to preserve motor function and D2 antagonist-like drugs are used in the treatment of Schizophrenia. Understanding the genotype of individuals affected with these conditions, then, could enhance the effectiveness of their D2 drug treatments (by suggesting a physician might want to start with a higher or lower dose of the drug). While studies such as ours linking genetic variation with differences in biology are encouraging, DNA can also be modified by the environment. Researchers have begun studying these epigenetic effects on behavior, with most work occurring in rodents. As we integrate this knowledge, we will begin to better understand the impact gene by environment interactions have on biology and behavior.
Non-genetic factors also influence dopamine signaling
Genetics are not the only variables that could be worth attending to in future treatments. Additionally, dopamine signaling is known to decline with age (see also a previous blog post on this topic). So, doses of dopaminergic drugs that work well on young adults might need to be titrated in older adults. Furthermore, we and others have shown that estradiol levels in naturally cycling women can affect dopaminergic brain functions (assessed by fMRI imaging and a genetic variant (COMT) know to affect dopamine levels in the higher-order, prefrontal areas of the brain). Thus, a dopaminergic medication might be more effective at treating a female patient’s symptoms at certain points of her menstrual cycle but not others. We are only beginning to understand the role of female sex hormones in a variety of biological systems as basic research historically has focused on male model organisms.
Dopamine signaling complexity and developing future treatments
The role of dopamine in drug addiction is quite complex. In addition, implementing personalized medicine when treating psychiatric or behavioral disorders is challenging as most of these disorders do not have a single, identifiable biological cause. The brain is complex enough and the fact that genetics, sex hormones, age, and environment can all affect one neurotransmitter (dopamine) among the many others involved in brain function speaks to the vast challenge that lies ahead for researchers.
Our quest to better understand individual differences, however, has the potential to lead to more targeted treatments and therapies for a variety of dopamine-associated disorders including ADHD, Schizophrenia, Parkinson’s Disease, and drug addiction. The development of these personalized treatments will undoubtedly improve healthcare in the 21st Century and beyond but will require further research focused on measuring and categorizing individual differences.
Our quest to better understand individual differences, however, has the potential to lead to more targeted treatments and therapies for a variety of dopamine-associated disorders including ADHD, Schizophrenia, Parkinson’s Disease, and drug addiction. The development of these personalized treatments will undoubtedly improve healthcare in the 21st Century and beyond but will require further research focused on measuring and categorizing individual differences.
Explore more neuroscience-related posts on the blog:
More scholarly articles on dopamine and its effects:
- Declining Dopamine: How aging affects a key modulator of reward processing and decision making
- Stress & the Brain: How genetics affects whether you are more likely to wilt under pressure
- Wanting, Liking, & Dopamine's Role in Addiction
- Now vs Later - How immediate reward selection bias may be a risk factor for addiction
More scholarly articles on dopamine and its effects:

















 RSS Feed
RSS Feed
{kind=link}